![The Real Costs of Restructuring at the WHO: Financing, Staffing and Mandates [WHA79 PRIMER]](https://storage.ghost.io/c/3e/27/3e275aa8-3271-4edb-ac7b-04dcacf8a053/content/images/size/w1280/format/webp/2026/05/pexels-steve-13659333.jpg)
Newsletter Edition #344 [The Files In-Depth]
Dear Readers,
Global Health Geeks are divided into two communities (among many others!), those who stay up to read financing docs from institutions, and those who do not. We are firmly in the former camp. Few things are more captivating than looking at balance sheets (ok, more than a few things)!
We bring you a primer ahead of the World Health Assembly that begins in Geneva next week.
This edition gets you up to speed on the implications of what the restructuring and realignment at the WHO has meant for the organization's mandate as a result of deep funding cuts in 2025. Indicators on finance and staffing have implications for governance in the context of such a realignment of the organization's priorities. Countries will review these matters next week at the Assembly. This edition includes an update on the elections process for the next Director-General of the WHO.
We hope you find this handy to have a quick look at the essentials before Assembly begins. This is Part I of a two part-primer. More from us in the coming days.
Geneva Health Files offers value to our readers who are experts in global health. Tracking global health policy-making in Geneva is tough and expensive, without institutional support. For six years, we have provided you with the information and tools that directly contribute to your work in the field. We rely on our readers who value news they can use.
By becoming a paying subscriber you make our work possible. Our subscribers contribute towards greater accountability in global health.
Best.
Priti
Priti Patnaik, Founder & Publisher, Geneva Health Files
Feel free to write to us: genevahealthfiles@gmail.com ; Find us on BlueSky, Instagram and Linkedin.
Presenting our weekly in-depth analysis on global health that captures the big picture and the nuances like no one else does. This is an exclusive edition for our subscribers.

I. GHF WHA79 PRIMER
The Real Costs of Restructuring at the WHO: Financing, Staffing and Mandates
By Priti Patnaik
Kavishalinie Kanagasabai contributed to this report
There are four segments to this edition: Finance, Human Resources, the Membership Question, and the Elections for a new Director-General.
We have distilled multiple documents, and cite graphs, tables to make all of this more accessible.
Key Takeaways:
- Funding cuts reveal deep impact on WHO's numbers. For the year ended December 2025, contributions from countries have been lower than the year before (2024). Many countries continue to pay their membership dues late. (Assessed contributions from countries accounted for 13% of revenue.)
- Voluntary contributions were 83% of the total revenue.
- Of the voluntary contributions of US$ 2567 million (to the programme budget), 8% was fully flexible or thematic, and was earmarked for specified programmes.
- The WHO has had to review and suspend some areas of work following funding cuts triggered by the United States. (See table below)
PART I: Finance:
- According to the WHO, "Financial pressures for the Organization continued in 2025, driven primarily by nonpayment of assessed contributions and suspension of voluntary contributions by the United States of America, which were mitigated by the implementation of strict cost containment measures."
- As per the audited financial statements for 2025, revenues decreased to US$ 3138 million (2024: US$ 3172 million), and expenses decreased to US$ 3429 million (2024: US$ 3763 million).
- In 2025, expenses exceeded revenue. (But WHO explains that "finance revenue of US$ 252 million reduced the net deficit to US$ 39 million (covered by accumulated surplus from previous years)."
- As before 83% of the revenue was accounted for by voluntary contributions (US$ 2600 million)
- Assessed contributions accounted for 13% of revenues.
- In 2025, assessed contributions fell by US$ 58 million. WHO says, "This reduction was driven by the increase in the movement in the allowance for doubtful accounts receivable (US$ 35.7 million) and a decrease in revenue due to the impact of the Swiss franc and US dollar exchange rate between January 2025 and January 2024 (US$ 22.5 million).
- WHO clarification on doubtful account receivable: "The allowance for assessed contributions receivable – current includes: (i) all amounts receivable from prior years; (ii) rescheduled assessments currently due; and (iii) amounts due for the current year from Member States in arrears to an extent that would justify invoking Article 7 of the Constitution, less any subsequent payments received before the preparation of the financial statements. The allowance for assessed contributions – non-current includes all non-current rescheduled assessments. The provision includes amounts due from the United States for 2024 and 2025 assessed contributions."
- Dues from countries funded 17% of the base segment of the Programme budget 2024–2025.
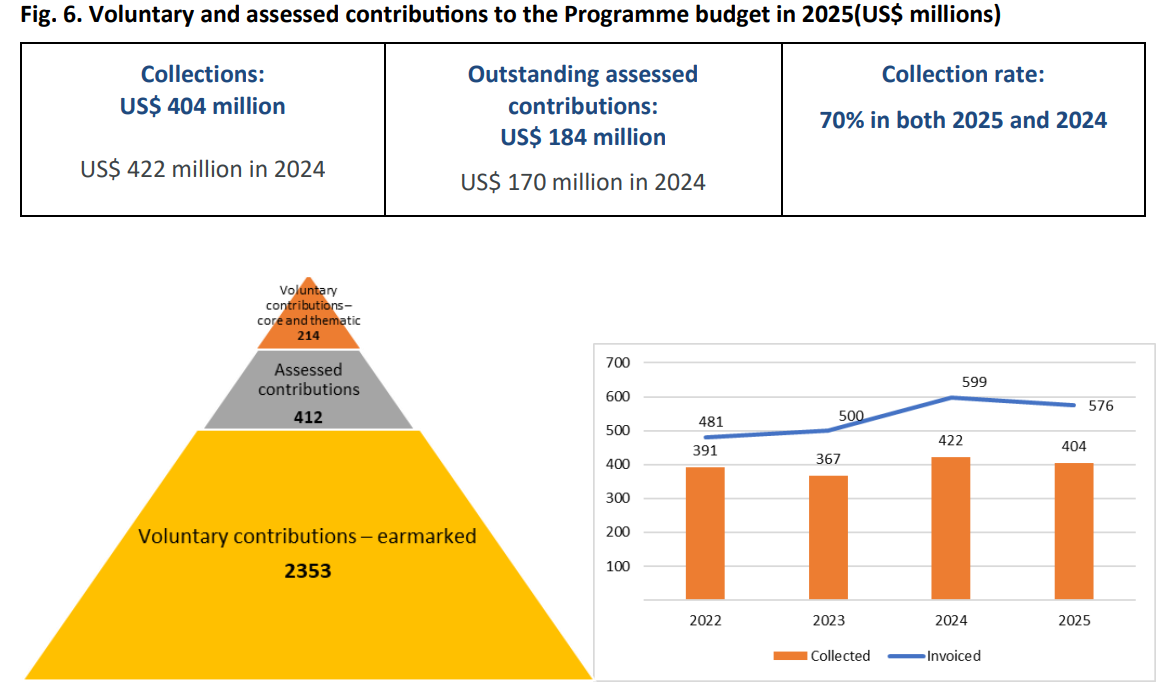
- Whats due? "Outstanding assessed contributions for the current year rose to US$ 184 million." While 75% of the 2025 unpaid amount is attributable to the United States, 46 Member States did not pay their 2025 assessments within the year.
- WHO says, "Assessed contributions from Member States are payable at the start of each year. These contributions are essential for timely and predictable financing of the Organization, especially during the current period of heightened uncertainty. They help to finance Member States’ priorities and provide catalytic funding to mobilize additional voluntary contributions....Member States are encouraged to improve the timeliness of their payments and reduce the amounts still outstanding."
- WHO said: "Flexible funding was US$ 626 million (21% of Programme budget revenue), a fall of 21% from 2024 (US$ 788 million or 26% of Programme budget revenue)." Contributions to the core voluntary contributions account decreased by US$ 170 million, and thematic funding increased by US$ 66 million.
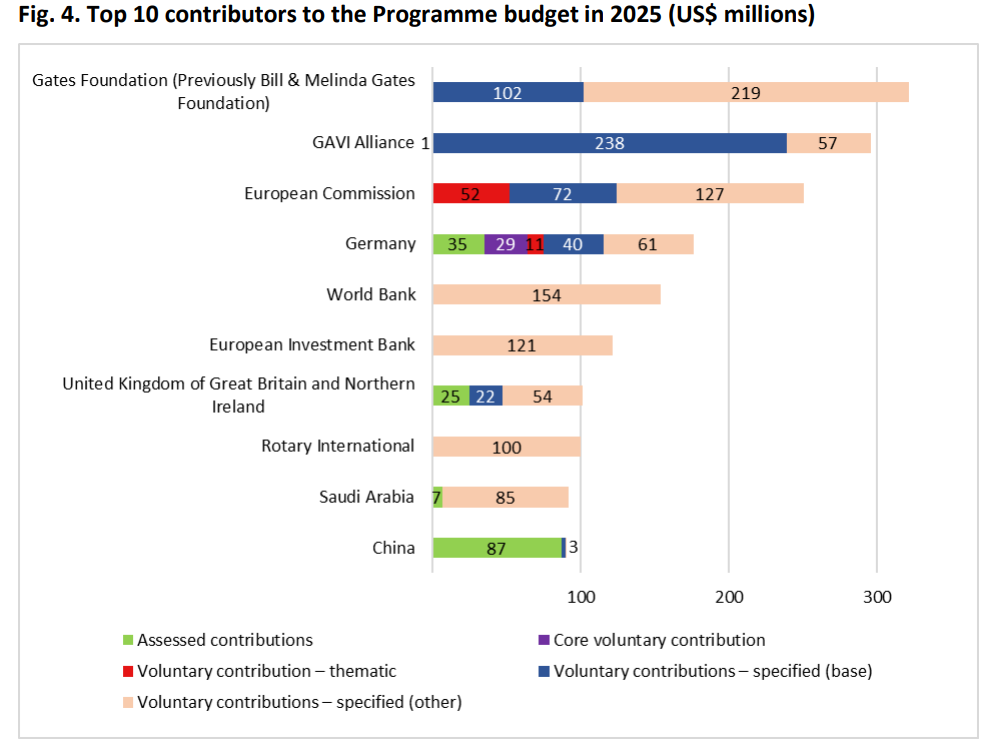
- The total contributions from the top ten donors to the Programme budget
amounted to US$ 1703 million, or 57% of contributions.[(Of this, US$ 247 million (14%) was fully flexible or thematic funding (including assessed contributions)] - How the voluntary contributions stack up: "Of the total revenue from Programme budget voluntary contributions of US$ 2567 million, US$ 214 million (8%) was fully flexible or thematic (designated to support high-level outcomes), and US$ 2353 million (92%) was earmarked for specified programmes," WHO said.
- Voluntary contributions to the Programme budget from Member States continued to fall, decreasing by US$ 175 million to US$ 926 million in 2025. They constituted 36% of total voluntary contributions to the Programme budget, a drop of 8% compared with 44% in 2024.
- WHO says: "Member States funding to the Programme budget peaked at 62% in 2022 during the coronavirus disease (COVID-19) pandemic, and this proportion has decreased in the years subsequent to the pandemic. A further contributory factor in the recent decrease has been the impact of the cessation of funding by the United States of America."
- Large volume of smaller agreements: "In 2025, the Organization received revenue through approximately 1250 agreements for Programme budget voluntary contributions (2024: 1200). Of these, 58 contributions were US$ 10 million or more and totalled US$ 1189 million. The remaining US$ 1267 million, 52% of gross voluntary contributions were contributed through over 1190 agreements."
- On dipping into reserves: Last year countries authorized WHO to partially and temporarily suspend Financial Regulation VIII, 8.2, enabling WHO to use Programme Support Costs Fund balances – up to US$ 410 million – to reimburse indemnities and salaries needed to support organizational realignment and ensure financial stability. This temporary suspension, effective through the second quarter of 2026, WHO has explained. (The Programme Support Cost (PSC) Fund, finances administrative and operational support activities. The PSC Fund generated significant revenue through support-cost charges applied to voluntary contributions.)
- Corporate reserves decreased from US$ 689 million in 2024 to US$ 631 million in 2025.
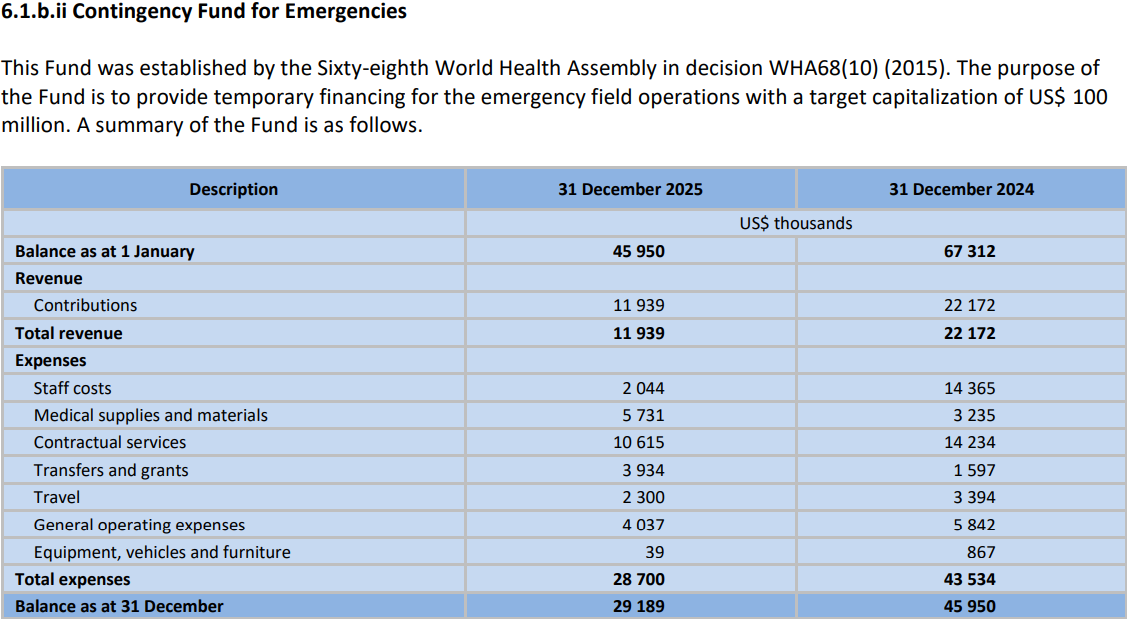
- One the biggest hit from the funding cuts is most evident for WHO's emergencies work. WHO said, "The Contingency Fund for Emergencies, established to support emergency health operations, experienced reduced balances due to high emergency-related expenditures. Spending covered staff deployment, medical supplies, contractual services, travel, and emergency response activities."
- Tailpiece: A note from the auditors
"Performance audit of resource mobilization (pipeline to agreement
management) in WHO
Justification for lost opportunities
• Out of 7016 opportunities, 556 cases (USD 1.59 billion) were marked as lost without recorded reasons - prevents analysis of failed engagements & weakens learning and accountability.
• Recommendation: Assess feasible system adjustments in the contributor engagement management (CEM) system to reinforce early recording of
opportunities to improve pipeline visibility in the CEM and coordinated donor engagement."
Updated with response from WHO, May 15, 2026:
"As WHO strengthens the practice within the CEM system of capturing potential funding opportunities at an earlier stage, it is expected that not all opportunities recorded in the pipeline will ultimately result in signed agreements. This is inherent to pipeline management, particularly when opportunities are captured early to support visibility, coordination and strategic engagement across the Organization.
At present, the system does not consistently capture the specific reasons why some opportunities do not materialize. This should therefore not be interpreted as donors reneging on commitments but rather reflects the inclusion of early-stage opportunities in the pipeline.
The recommendation from the auditors is aimed at further strengthening the analytical value of the system by enabling more systematic tracking of outcomes and lessons learned from engagement efforts."
PART II: HUMAN RESOURCES
- The financial crunch and restructuring, led to a near 10% drop in WHO’s total workforce to 8569 in 2025, according to a report on human resources by the DG.
- According to WHO, the number of consultants fell by 22%, from 5317 (1717 full-time equivalents) in December 2024 to 4148 (1280 full-time equivalents) in December 2025, representing a 25.5% drop in full-time equivalents. (See workforce data here)
- Staff costs: In 2025, staff costs amounted to US$ 1228 million and increased as a percentage of total expenditure, to 36.0% of US$ 3429 million from 34.0% of US$ 3762 million in 2024. (Staff costs fell in absolute terms by 5% to US$ 1.23 billion.)
- According to WHO, by 30 June 2026, the number of WHO’s global staff is projected to reach 7283 ‒ a 23% reduction compared to the number of global staff as at 1 January 2025 (9401) – based on remaining staff members. (Approximately 368 additional vacant positions are being prioritized.)
- On geographical diversity: 66% of countries are well represented, while 34% are un/underrepresented.
- WHO has new plans on making workforce more inclusive, including secondments: "Secondments – new secondments available from 1 July 2026 Secondments enhance collaboration and knowledge exchange, offering exposure and pathways to longer term opportunities." (Not clear to us yet on how this will work and from which institutions)
- On mobility: "The ongoing financial crisis has had a direct impact on WHO staff mobility frameworks, particularly the Global Geographical Mobility Policy. The 2025 mobility exercise could not proceed as planned owing to organizational restructuring and resource constraints. Staff members continued to be moved, however, notably through the global reassignment process, which is used to identify viable placement opportunities for eligible staff whose positions are abolished during prioritization and realignment, and the normal channels of reassignment, both within and across regions, including relocation of positions as part of the restructuring process....While the Global Geographical Mobility Policy is paused, WHO continues to uphold mobility principles in practice, prioritizing internal talent retention, filling essential roles at country level and ensuring continuity of operations. The Organization is also reviewing how and when to re‑launch the mobility initiative once the financial situation stabilizes."
Impact on mandates: WHO’s prioritization and realignment
In a document to be considered next week, WHO lays out the impact of the restructuring and realignment. (It also clarifies: "This report is presented as an exceptional contribution to ensure that the Executive Board and governing bodies are provided with sound and timely information, recognizing that the current situation requires an exception to the standard reporting modalities..."
We had reported on the restructuring process earlier in the year during the Executive Board meeting in January 2026. Recall that in 2025, WHO's budget for 2026-2027 was slashed by 21% to US$4.2 billion from what was originally proposed. This led to massive restructuring of the organization, and resulting activities. Last year, a new headquarters structure was announced that restructured from 11 to six divisions and from 67 to 36 departments.
In WHO speak, this means:
"The prioritization of programmatic priorities, roles and responsibilities, was guided by a refocusing on WHO’s core mandate."
"The Secretariat initiated a thorough review of all deliverables against the Proposed programme budget 2026‒2027 (which is aligned with the Fourteenth General Programme of Work (GPW 14), 2025–2028) in order to determine what to sustain and strengthen, what to scale down or stop, and where to improve efficiency and impact. This resulted in the allocation of budget envelopes to all budget centres in every major office, covering both human resources and non-staff costs, which were considered when designing the new Organizational structures.
Organizational realignment activities were implemented in accordance with the approved budget envelopes and applied comprehensively across all three levels of the Organization..."
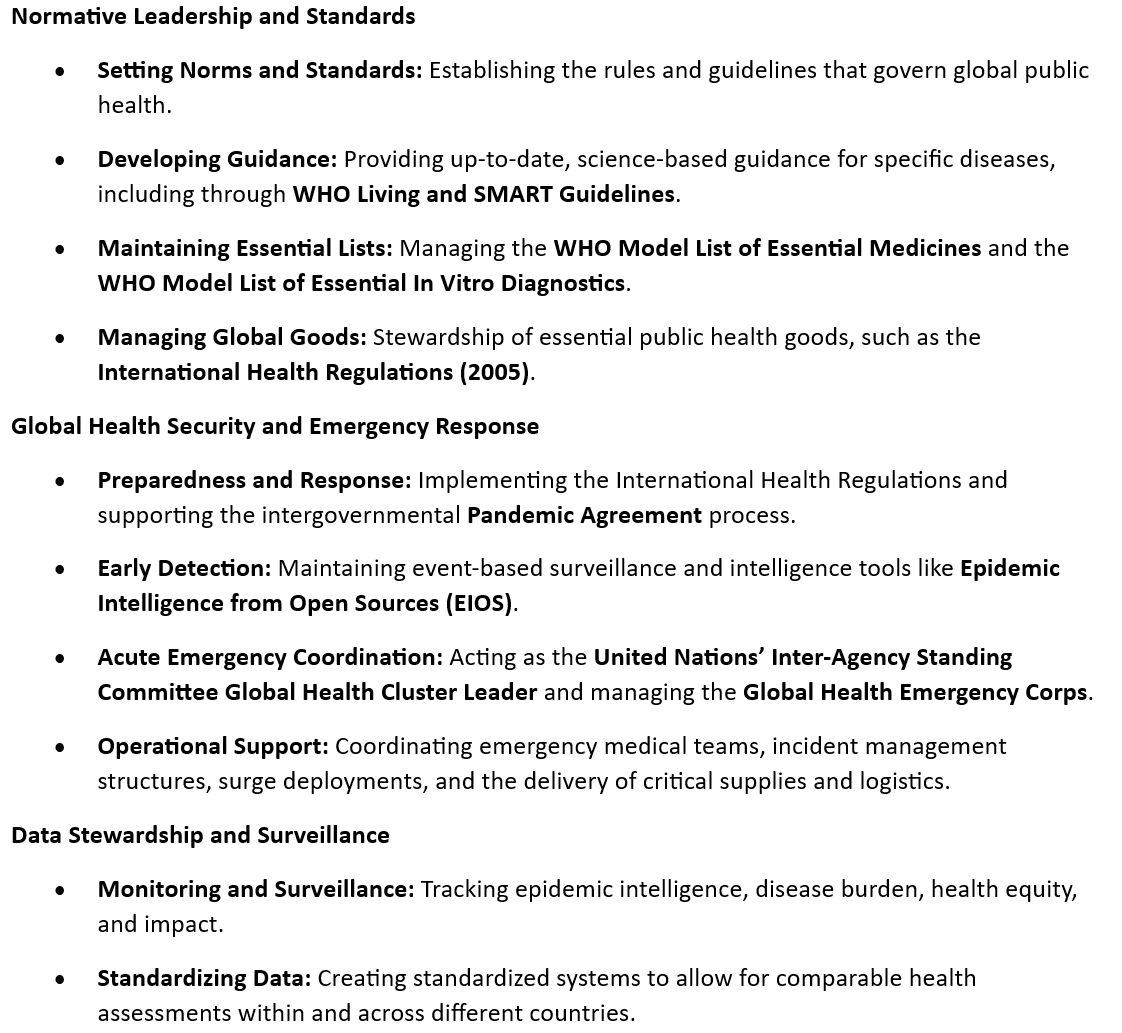
Scale down and stop: stopping or sunsetting activities at the divisional/departmental levels against defined criteria
In its update, WHO has said:
"This dimension ensured that resources are focused on WHO’s highest‑value functions....Activities have been reduced or discontinued where they were obsolete, duplicative, better delivered by others, primarily operational/implementation in nature or of minimal strategic utility.
These examples are illustrative and non-exhaustive, reflecting the application of consistent criteria across diverse technical and functional areas, while preserving WHO’s core normative, convening and stewardship roles."
Source: WHO, May 2026:
|
Where
work was no longer strategically relevant, WHO has stepped back (Examples)
•
discontinuing direct scientific leadership of selected clinical trial
platforms, such as tuberculosis trial platforms and multicountry newborn‑health
trials, while reinforcing its normative role on trial standards, ethics and
inclusion; •
discontinuing selected legacy technical platforms, tools, assessments and
stand‑alone initiatives whose original purpose has been fulfilled, with WHO
retaining a standards‑setting, guidance and quality‑assurance role rather
than direct operational ownership; and •
rationalizing disease‑ or event‑specific response tools developed for earlier
emergencies, as capacities are integrated into more sustainable, cross‑cutting
preparedness and surveillance architectures. |
Where
mandates lie more clearly with other United Nations agencies, WHO has reduced
overlap (Examples) • scaling
back Secretariat support to external multipartner United Nations mechanisms
in which mandates and coordination functions are now more clearly anchored
elsewhere, such as in selected inter-agency platforms and trust-based
coordination structures, allowing WHO to focus on its comparative normative
and technical roles; and •
clarifying lead roles in protection‑adjacent or protection‑linked thematic
areas, with WHO stepping back from parallel delivery, while continuing to
provide technical guidance and standards where health mandates remain
relevant ‒ for example, in selected areas of menstrual health, sexual and
reproductive health in humanitarian settings, and related protection work now
led by the United Nations Population Fund and the United Nations Children’s
Fund. |
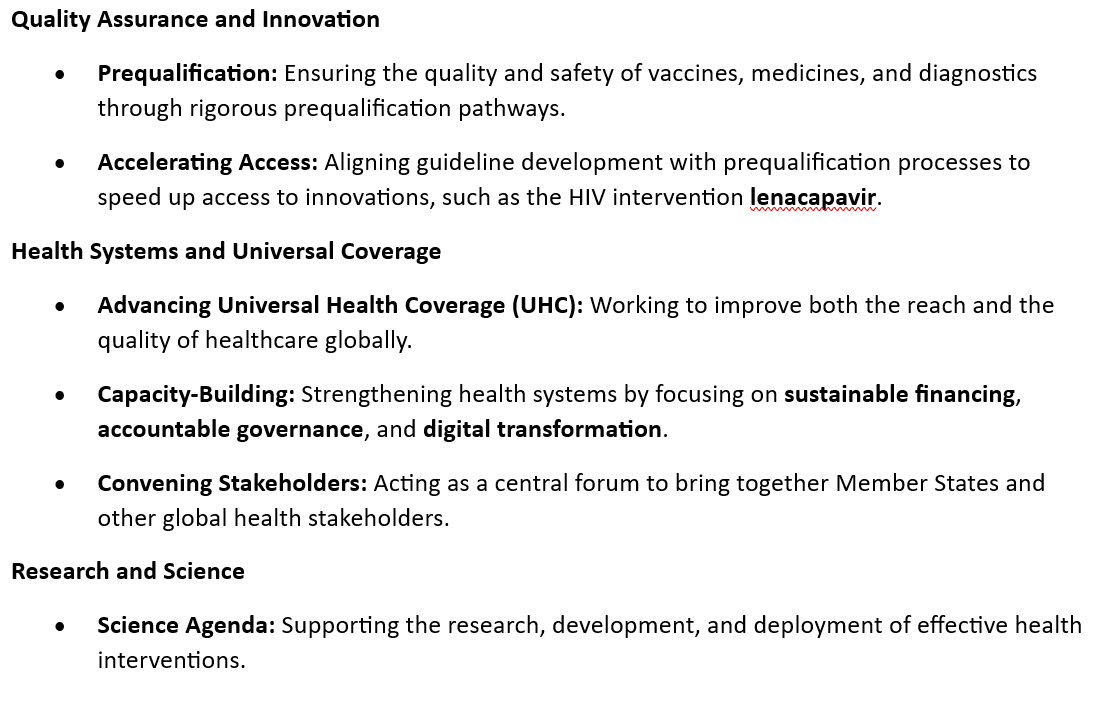
Where
other partners can deliver more effectively at scale, WHO has transitioned
work (Examples) • handing
over logistics functions to operationalize appropriate transfer of innovative
technologies and support geographically diversified health product
manufacturing capacity; •
transitioning selected training, learning and operational‑innovation
activities ‒ including selected innovation hub initiatives (demand Catalyst
and LEAD) ‒ to the WHO Academy and WHO collaborating centres, thereby
consolidating delivery while maintaining WHO stewardship over quality and
normative alignment; and •
refocusing community-level or country-level implementation activities towards
policy guidance, advocacy and partnership enablement, where national
authorities and implementing partners are better placed to deliver at scale. |
Where
WHO can step back, while stepping up where it must, WHO has refocused its
resources as follows: • in acute
emergencies, WHO differentiates between roles best performed through
coordination and normative guidance and those best performed through direct
delivery, stepping back from operational functions where countries and
partners are able to lead, while stepping up its unique convening, standard‑setting
and operations role where gaps in knowledge are clear or emerge and no
alternative capacity exists; • WHO’s
technical assistance to countries is increasingly differentiated, with more
intensive engagement concentrated on priority and fragile contexts, while
lighter‑touch, demand‑driven support, including to coordinate contributions
of other partners, is applied elsewhere. |
Where
strategic utility was limited, WHO has streamlined internal outputs,
(Examples) • streamlining or discontinuation of
publishing, reporting and internal knowledge products, reducing volume and
frequency (e.g., stopping non-mandated publications in the WHO Health
Emergencies Programme), while safeguarding the quality and integrity of WHO’s
normative and flagship outputs; •
decommissioning selected in‑house digital platforms, tools, apps and
analytical products, where equivalent or superior solutions are available, with
WHO shifting to stewardship and validation roles; and • reducing
the number of stand-alone technical products (e.g., in the areas of
environment, climate change, One Health and migration), while prioritizing integrated,
higher‑impact guidance outputs aligned with the GPW 14 and country demand |
PART III: MEMBERSHIP TO THE WHO [Argentina]
A member state briefing on the sensitive issue of the membership of Argentina suggests that the Assembly approve the resolution from the EB on the matter.
According to an update from WHO:
"• On 17 March 2025 – Argentina notified the UN Secretary-General of its denunciation of the WHO Constitution.
• 21 April 2025 – The UN Legal Counsel informed the WHO Legal Counsel of the notification. She indicated that since the WHO Constitution does not contain any provision on denunciation or withdrawal, the depository was not in a position to determine whether the notification can be accepted in deposit and indicated that the depository will be guided by the Health Assembly in regard to this matter. She requested that the matter be brought to the attention of the Health Assembly. Consideration by the Governing Bodies to date
• WHA78 considered the Secretariat’s report (WHA78/33 Add.1) and requested that these matters be considered at EB158 and WHA79 (decision WHA78(25)).
• EB158 noted the Secretariat's report (EB158/45) and adopted Decision EB158(12) on "Withdrawal of the Argentine Republic from the World Health Organization", recommending that WHA79 adopt a draft resolution on the matter.
• If adopted by the Health Assembly, that draft resolution would “acknowledge the withdrawal of the Argentine Republic from the World Health Organization, effective as of 17 March 2026." Consideration of this Matter at WHA79
• Item 20.2 "Communications of the United Nations Secretary-General as depositary of the Constitution of the World Health Organization". (Provisionally scheduled for Friday, 22 May, in Committee B.)
• WHA79 will be invited to consider the draft resolution recommended by the Board in decision EB158(12) (2026)"
(See our recent analysis on this: What The Creative Ambiguity Around The Withdrawal From The World Health Organization Means)
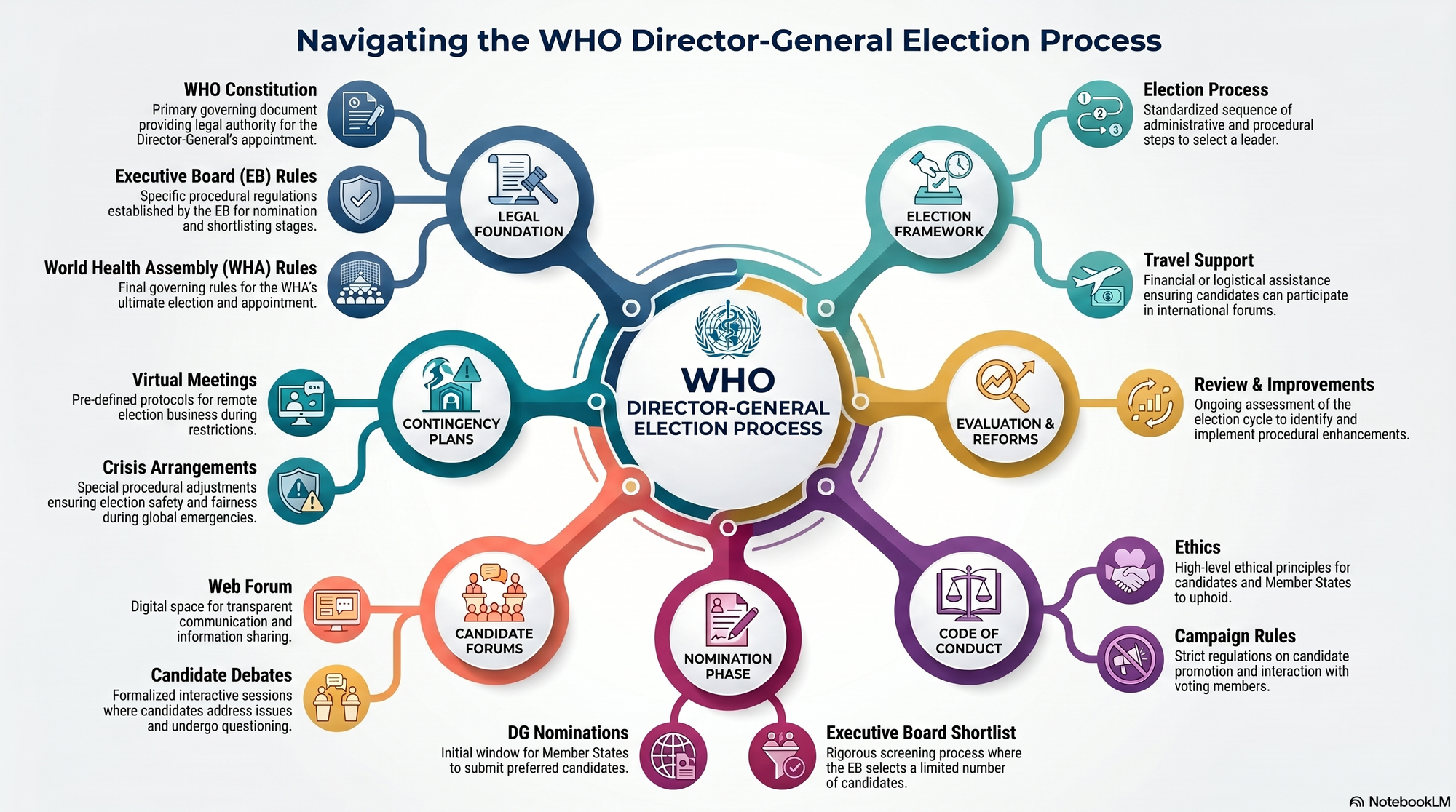
PART IV: THE PROCESS FOR THE ELECTION OF THE NEW DG
- WHO has also published a map and a timeline to inform the process of the election of the next Director-General.
- The process for the election of the Director-General is governed by the Constitution of the World Health Organization, the relevant rules of procedure of the World Health Assembly and the Executive Board, as well as several resolutions and decisions of both these organs, WHO has said.
It lays out certain parameters for the process:
- The dates of and detailed arrangements for the candidates’ forums
- Travel support to candidates attending the interviews at the session of the Board at which the nomination will take place
- The status of internal candidates
- Electoral campaign activities at sessions of the regional committees.
Candidates' Forums
- As per rules, two candidates’ forums will be convened by the Secretariat as stand-alone events to enable the candidates for the post of Director-General to make themselves and their vision known to Member States on an equal basis. (Both forums are non-decision-making platforms open to all Member States and Associate Members, and are broadcast on the WHO website, the WHO has said)
- The first candidates’ forum shall be held not later than two months before the opening of the session of the Board at which the nomination will take place.
- The second candidates’ forum shall be held not later than two months before the opening of the Health Assembly at which the appointment of the Director-General will take place.
- (The EB will decide the dates of the forums at its session preceding the session at which the nomination will take place.)
"(a) Should the Board agree with the proposal contained in document EB159/13 to convene the 160th session of the Executive Board on Monday, 25 January to Tuesday 2 February 2027, the first candidates’ forum shall be held no later than 24 November 2026. It is therefore proposed to convene the first candidates’ forum starting on 18 November 2026.
(b) Should the Board agree with the proposal contained in document EB159/13 to convene the Eightieth session of the World Health Assembly from Tuesday, 18 May to Wednesday 26 May 2027, the second candidates’ forum shall be held no later than 17 March 2027. It is therefore proposed to convene the second candidates’ forum on 15 March 2027."
- "Each candidate will make a presentation of up to 10 minutes, to be followed by a question-and-answer session, amounting to an overall duration of each interview of 60 minutes.
- The second candidates’ forum will consist of an interactive panel discussion between the candidates and Member States and Associate Members attending the forum.
Prospective candidates
- "Given that the official announcement of candidates for the post of Director-General will take place after the closure of the last regional committee session before the session of the Executive Board at which the nomination will take place (that is, on or after 29 October 2026), and in order to promote transparency and equality of opportunity for all persons who are or may become candidates, persons who have been or may be proposed as candidates may be acknowledged as prospective candidates prior to the aforementioned official announcement of candidates. Prospective candidates will be acknowledged on the WHO website."
- "Acknowledgement of a person as a prospective candidate will take place at the request of a Member State. In addition, if any internal candidates are not already acknowledged as prospective candidates, they will also be acknowledged as prospective candidates as soon as possible following the opening of proposals."
On Internal candidates
- "...In accordance with Staff Rule 650.2 and paragraph IV.4 of the Code of Conduct for the election of the Director-General of the World Health Organization,7 the Director-General intends to place internal candidates on special leave to ensure a clear separation between their campaign activities and WHO’s functions"
WHA79 EVENT: HEALTH DIPLOMACY HOUSE
The Health Diplomacy House is an informal, practical co-working open space where organizations convene sessions, hold discussions, and work on concrete health policy issues. As part of the Predictable Uncertainty series, it brings together policymakers, diplomats, academia, youth, civil society, philanthropic actors, the private sector, and patient groups to establish workstreams beyond the Assembly.
Global Health Architecture and Governance: Reflection in an Era of Predictable Uncertainty
This session will set the tone for all partner organization sessions within the Health Diplomacy House, connecting the Alliance's strategic priorities — including AMR, climate change and health, health governance, and sustainable financing — to wider global reform processes. It is designed as a space for reflection that goes beyond standard exchanges, fostering meaningful dialogue on how current shifts shape the future of international health cooperation.
Check the Box: AMR
This session will focus on tracking political commitments on antimicrobial resistance, assessing the gap between declaration and implementation, and identifying the diplomatic and policy levers needed to accelerate action — turning high-level commitments into concrete accountability.
Also from us:

Global health is everybody’s business. Help us probe the dynamics where science and politics interface with interests. Support investigative global health journalism.







