
First published on January 21, 2026, this edition has been updated with information around developments of the U.S. withdrawal from WHO, and information on governance reform.
Hi,
Board meetings are a good time to plant the germ of reforms, and to see what happens. And be sure, that things will take shape and happen.
WHO is calling for a multi-stakeholder, inter-agency process for reforms in the Global Health Architecture.
In this 4,000+ word edition, we bring you a primer on what’s coming up at the WHO Executive Board Meeting early next month.
The goal has been to capture the most important elements on governance, financing and the strategic stuff, that will be considered at this important annual event in the Global Health Geneva calendar. We intend this to be a quick primer for our readers - most key issues all in one place.
We are also having a timely workshop next week where we will walk through some of these matters and discuss behind-the-scenes deliberations. Register here! (This is a free offering for our subscribers! If you are a subscriber interested in the session, just send me an email.)
Geneva Health Files strives to offer value to our readers who work in global health. But it is hard to do this without institutional support, so we rely on our news they can use.
Support public interest global health journalism, become a paying subscriber. Tracking global health policy-making in Geneva is tough and expensive. Help us raise important questions, and in keeping an ear to the ground. makes this possible.
Gratitude to our subscribers who help us contribute to greater accountability in global health.
More soon!
Best,
Priti
Feel free to write to us: genevahealthfiles@gmail.com; Find us on BlueSky: https://bsky.app/profile/genevahealthfiles.bsky.social

I. GHF ANALYSIS: EB158 PRIMER
Financing & Governance at a Restructured World Health Organization: A Primer on the 158th Executive Board Meeting
WHO Pitches For A Multi-Stakeholder Inter-Agency Process For Global Health Architecture Reform
In this comprehensive briefing, we bring you a quick overview of key financing and governance issues that will come up at the WHO Executive Board early next month. I reviewed the docs, distilled, and cited relevant excerpts for you on some of the key issues to watch out for.
Also, check out below, WHO’s plans to host “an overarching, joint process that brings together current Global Health Architecture reform discussions, and UN80 proposals with potential implications for global health”.
It is suggesting a multi-stakeholder, inter-agency process similar to the ACT-Accelerator during COVID-19, and proposes to “consult” countries on this. The way such an initiative will be “managed” will be important, given WHO’s distinguishing role as a member-state led institution. (We are trying to find out more on this, not all diplomats seemed to be aware of such an initiative in the works.)
PART 1: GOVERNANCE & OTHER AGENDA ITEMS
I. WHO STAFFING MATTERS
WHO’s prioritization and realignment process in 2025
- When Donald Trump announced withdrawal from WHO a year ago on January 20, 2025, within days, member states negotiated a reduction in the size of the organization’s budget for 2026–2027 from US$ 5.3 billion to US$ 4.9 billion. This was subsequently whittled down to US$ 4.2 billion, “based on the further assessment of the financing landscape, which was approved by the Seventy-eighth World Health Assembly in May 2025,” the report from the DG says. This was a 21% reduction from the original proposed programme budget.
- “To operate within the reduced budget while preserving WHO’s core mandate, the Secretariat undertook a strategic prioritization and realignment process to define essential functions and align financial and human resources accordingly,” the report says.
- Recall that in 2022, countries agreed to gradually increase their assessed contributions to represent 50% of WHO’s core budget by the 2030–2031 budget cycle. So while this increase from membership dues have helped, the withdrawal of the U.S. and the non-payment of its dues added to the gap in funding. (“The total planned assessed contributions for 2024–2025 have been revised down from US$ 1,148 million to US$ 885 million. Assessed contributions already made available for implementation had to be withdrawn from programmes,” WHO says.)
- The U.S. also withdrew voluntary funding across key areas, exacerbating the crisis. WHO notes that the U.S. funding has not been “replaced”: areas impacted by US funding withdrawal continue to face gaps. In addition, earmarking limits flexibility, that is funds cannot be shifted to areas with shortfalls, WHO said in recent a member state briefing.
How the management guided the restructuring:
- In the document, WHO explains:
“The Secretariat outlined a distinct methodology based on three foundational considerations to guide the design and implementation of the prioritization and realignment process:
(a) the prioritization of programmatic priorities, roles and responsibilities was guided by a renewed orientation in line with WHO’s core mandate. The Secretariat initiated a thorough review of all deliverables against the Fourteenth General Programme of Work, 2025–2028, to determine what to sustain and strengthen, what to scale down or stop, and where to improve efficiency and impact. This included a financial analysis that resulted in the allocation of funding envelopes to all major offices covering both human resources and non-staff costs which were considered when designing the new organizational structures;
(b) organizational realignment activities were implemented in accordance with the approved budget envelopes and applied comprehensively across all three levels of the Organization;…”
The report also adds that “the design of the process was anchored in three core principles: transparency, fairness and humanity.”
How the decision of budgetary allocation was made across the organization and at the various divisions at the headquarters is understood to be a managerial determination, sources say. The financial analysis underpinning the restructuring is not public, but is said to be based on the outcome of the prioritization process.
How the restructuring was conducted:
The prioritization and realignment process was conducted in four phases, WHO says [excerpts]:
“Phase 1: Structure definition. The high-level and detailed organizational design exercise began by defining a new headquarters structure, moving down to 6 divisions and to 36 departments by identifying significant opportunities for synergies through mergers subsequently consolidating units, teams and positions to create a more efficient structure. This resulted in a substantially leaner leadership team (a reduction by 50%)….
Phase 2: A “mapping and matching” realignment exercise. This began once the organigramme and associated human resources plan had been approved by the Director-General for headquarters and by the Regional Directors for their respective major office. Individuals were then (a) neither mapped nor matched; or (b) mapped or matched to positions based on role alignment with their current functions. This process was applied to all staff in active service holding continuing or fixed-term appointments.
Each division and regional office convened an ad hoc review committee (ARC) to review all mapping and matching proposals. The ARC meetings included an independent member and a WHO staff association representative. Beyond the ARC work throughout the mapping and matching phase, staff members were invited to direct any concerns to a transparency and fairness committee established in each major office
Phase 3: Individual communications. Individual meetings were conducted with staff members who had not been mapped or matched to a position, or where their position had been relocated to another duty station.
Phase 4: Reassignment process. Reassignment committees were activated for staff who were neither mapped nor matched to a position in the new structure yet were eligible for the formal reassignment process. These individuals were supported in identifying suitable vacancies across the Organization during the reassignment period in accordance with Staff Rule 1050. The reassignment process has been centrally managed by headquarters for international staff and by major offices for local staff. It is designed to last up to six months, during which eligible staff receive support in finding suitable vacancies across the Organization. This step is ongoing and, once finalized, will conclude the organizational structure review process.”
THE STATUS ON NUMBERS
- In the report to the Board, WHO said: “Since the beginning of 2025, WHO has adopted a deliberate approach to the prioritization and realignment process, favouring preventive measures. WHO successfully reduced the overall number of separations through measures such as natural attrition, retirement and voluntary early retirement involving a total of 1089 positions, while preserving approximately 600 positions thanks to the increase in assessed contributions. As a result, the Organization faced 1282 post abolitions.”
- “Overall, through this approach, approximately 46% of all global separations are being managed through preventive measures, while the remaining 54% of separations between January 2025 and June 2026 require invasive measures.The report notes: “…Nevertheless, preventive measures alone were not sufficient to fully realign the Organization with new operational and financial realities. Consequently, WHO had to complement these efforts with more active separation measures, applied carefully and only as a last resort, to ensure sustainability and continuity. Additional measures included separation by mutual agreement to enable early exits under mutually agreed conditions, as well as an extended one‑month notice period for temporary staff…”
- “By 30 June 2026, the number of WHO global staff is projected to reach 7360, representing a 22% reduction compared with 1 January 2025 (9401) based on the number of remaining staff members. It should be noted that approximately 1052 additional vacant positions are being maintained.”
- “If all these positions were filled, the headcount by 30 June 2026 would be around 8412, representing an 11% reduction from the January 2025 level. Overall, this reduction (between -22% and -11%) reflects a strategic shift towards a leaner, more agile Organization, better equipped to respond rapidly to emerging health challenges, allocate resources where they have the greatest impact and reinforce WHO’s leadership in an evolving global health landscape.”
- “Projected distribution of global staff by level: By 30 June 2026, the projected distribution of staff across the three levels of the Organization is expected to be 45.6% in country offices (+0.9 percentage points compared with January 2025), 25.9% in regional offices (+1.5 percentage points) and 28.5% at headquarters and Global Shared Services (-2.4 percentage points).”
- We recommend you read this short report. Acknowledges that they have made progress, but more remains to be done
- Notes “fear of retaliation”. Gap between official narratives and lived experiences
- Cautions about not enough ombudsmen in the organization.
STATEMENT FROM THE STAFF ASSOCIATIONS
(WHO, IARC, PAHO and UNAIDS) Excerpts:
- “The staff associations recognize the profound disruption caused by the prioritization and realignment exercise, which has affected personnel across all regions. These changes have not only impacted individual livelihoods but also risked eroding institutional memory and expertise – both of which are essential to WHO’s operational effectiveness and credibility.”
- “Staff continue to express disappointment at the limited transparency surrounding WHO’s strategic priorities and how these were translated into departmental structures, as well as the lack of explanation and rationale for certain decisions and the absence of information regarding job losses by grade and contract type. While this information was eventually shared with staff in the Director-General’s message issued the night before the Member States briefing, many colleagues had been requesting such clarity throughout the process to better understand the rationale for the sunsetting of their areas of work or the abolition of their posts.”
- “…Staff are concerned that it is not clear which tasks WHO staff will no longer be undertaking, given the reduced workforce. Equally, they are concerned that Member States still expect WHO to fulfil pre-crisis work programmes. Such expectations will invariably lead to increases in the numbers of consultant contracts, undermining an already tenuous contractual situation for many employees.”
- “We also note that during subsequent Executive Board discussions, several Member States and independent reviews highlighted the need for even higher levels of predictable assessed funding ‒ in the range of 60% to 70% of WHO’s core programme budget ‒ in order to ensure WHO’s long-term financial sustainability and reduce overdependence on highly earmarked voluntary contributions. It is in this context that the staff associations support efforts to strengthen the share of assessed contributions and call for greater transparency in the operations of the resource allocation committee.”
- “Staff associations must be able to participate in governance processes-such as meetings of the Global Staff Management Council – without being subject to the discretionary budget decisions of management. Staff are the Organization’s most valuable asset, as consistently recognized by both management and Member States, and ensuring that their representatives can participate meaningfully in these forums is not a privilege but a fundamental aspect of inclusive and transparent organizational governance. When participation is contingent on managerial discretion or funding availability, it undermines the independence of staff associations and compromises the integrity of dialogue between staff and leadership. We therefore call for the participation of a staff association representative in all governance meetings, ensuring that their voices are consistently heard and valued..”
WHO AND THE UN80 REFORMS
- The report provides an overview of the context for reforming the global health architecture (GHA) and the UN80 Initiative, and notes the proposals for GHA reform and potential implications for WHO.
- “The significant contraction in official development assistance (ODA) since its 2022 peak, particularly in 2025, combined with escalating pressures on the traditional multilateral order have placed new strains on international organizations both within and outside the United Nations system, countries, global health actors and the global health agenda. These developments are putting at risk recent global health successes, including: since 1990, the nearly 10-year gain in life expectancy globally, and the 60% and 40% reductions in under-5 and maternal mortality respectively; and, since 2000, the estimated 75 million, 25 million and 13 million deaths averted due to vaccine-preventable diseases, HIV and malaria respectively. Additional achievements include the 2005 entry into force of both the WHO Framework Convention on Tobacco Control and the International Health Regulations (2005) and the adoption in 2025 of the WHO Pandemic Agreement.”
ON THE REFORM PROPOSALS:
- “The contraction in ODA and ambition for a more relevant and impactful United Nations system, have led to multiple reform-focused initiatives. At the national level, countries have worked to increase domestic resources for health and better align donor financing with national priorities, in line with the Lusaka Agenda and the goals of the newly established Health Works Leaders Coalition….
- Major global health entities and organizations have also launched substantive reforms, including Gavi, the Vaccine Alliance, the Global Fund to Fight AIDS, Tuberculosis and Malaria, UNAIDS, UNFPA and UNICEF, in addition to WHO. These reforms include rationalizing programmes and structures to fit within new funding realities and focusing available resources where they are most needed. In parallel, both the UN80 Initiative and a number of discussions on the GHA have generated further reform proposals, some with potential implications for WHO. Together, these efforts have created momentum for rethinking the GHA for greater impact. Amid such profound change, ensuring coherence across these interrelated efforts is essential for synergistic action to advance global health and well-being.”
ON THE OPPORTUNITIES FOR WHO FROM THE UN80 PROCESS:
- “Regarding workstream 3, WHO was a member of the specialized agencies, development and humanitarian thematic clusters, contributing to proposals culminating in the United Nations Secretary-General’s report of 18 September 2025, Shifting paradigms: United to deliver.The report has potential implications for WHO and global health.First, through the proposed merger of UNFPA and UN-Women, the sunsetting of UNAIDS and the delegation of United Nations Secretariat functions to other entities of the United Nations system.Secondly, by expanding the role of specialized agencies at the country level through their inclusion in a new operating model for United Nations country teams, the reformulation of the Resident Coordinator role to more systematically engage them in country planning and policy advice, and the introduction of joint knowledge hubs and an “expertise-on-demand” mechanism.Thirdly, through the “regional reset” to enhance collaboration across United Nations entities at that level and the development of regional integrated platforms to advance cross-cutting issues.Fourthly, by taking forward the humanitarian-related action items, particularly those on integrated supply chains, the development of a collaborative humanitarian diplomacy initiative, and greater localization and streamlined coordination, including for health and nutrition….”
“Taken together, the UN80 Initiative proposals could expand WHO’s directing and coordinating work on health across the specialized, development and humanitarian domains of the United Nations system.”
WHO IN THE CONTEXT OF THE GLOBAL HEALTH ARCHITECTURE
- “Alongside the growing pressure on global health actors to refocus and rationalize resources, numerous initiatives, papers and discussions on GHA reform have emerged, examining issues such as rationalizing the international financing of both global public health goods and development cooperation for health at the country level; advancing country leadership, priorities and self-reliance for national health, in line with the principles of the Lusaka Agenda; strengthening regional coordination and capacities for health, including for health product manufacturing; and establishing meaningful global health governance and coordination across increasingly diverse constituencies. There is strong consensus that reform should be substantive, go beyond cost-saving measures and aim to make the GHA more equitable, inclusive, coordinated and accountable, with sustainable and predictable financing for key global, regional and national functions. These include norms and standards, surveillance and preparedness, product innovation and access, and the harmonization of financial cooperation through convening, coordination and, ideally, mutual governance.”
- “Ongoing initiatives include the Wellcome Trust regional dialogues on global health reform; the European Commission reflection process on the future of global health; the Gavi Leap radical transformation programme for a new global health architecture; the Accra Reset initiative on reimagining global governance for health and development; and the Health Architecture Reimagined initiative led by civil society organizations.”
- “The evolving proposals under the UN80 Initiative and the diverse perspectives emerging from discussions on GHA reform highlight the need for coherent and consistent outcomes. The Member State-guided WHO efficiency, prioritization and alignment exercise has emphasized WHO’s core functions; the UN80 Initiative has underlined WHO’s coordination of health actions in the specialized, development and humanitarian domains and the possibility of taking on additional functions; while discussions on GHA reform sometimes propose an even sharper focus for WHO in terms of its core functions.”
- “Optimizing the GHA, and WHO’s role in this new era, requires a common framework, in terms of the GHA’s purpose, major functions, actors and capacities. Such a framework could serve as a basis for guiding priorities, investment and enhanced collaboration modalities.Developing such a framework requires engaging all key constituencies that comprise the GHA, including countries, United Nations entities, global health initiatives, development banks, sovereign donors and philanthropies, product development partnerships, the private sector, civil society and academic institutions. As key actors and sponsors of the GHA, Member States have a central role in championing and helping to shape its reform.”
- “To facilitate deliberations on the future of the GHA, and in the context of UN80, WHO proposes to host an overarching, joint process that brings together current GHA reform discussions, and UN80 proposals with potential implications for global health, and complements them as needed with additional evidence gathering, research and consultation, to develop a common framework for the GHA.
- Such a joint process would build on lessons learned from similar WHO-hosted inter-agency processes, such as the Access to COVID-19 Tools Accelerator (ACT-A) during the pandemic. The process would be transparent, inclusive, and evidence based and generate common products that could be considered by all relevant entities. Initiating such a process in the first half of 2026 would help to align with the timelines of the UN80 Initiative and time-bound consultations on GHA reform. Member States would be further consulted on the design of the process, and thereafter kept informed on and engaged in the UN80 Initiative and the GHA consensus-building process through briefings and official updates, including through governing body processes as appropriate.”
WHO has requested countries to guide on: • how to design a joint process, hosted by WHO, that brings together and complements current GHA and UN80 discussions to facilitate convergence and consensus-building; and • how best to engage the full range of global health actors, including other global health entities, regional organizations, development banks, philanthropies, civil society and academic institutions.
ON THE U.S. & ARGENTINA
The board will also consider a report related to the notifications of withdrawal from the Organization from Argentina and the United States of America. This follows deliberations at the Assembly last year A78/33 Add.1
See report to the EB, where communication from the organization expounds on the legal considerations regarding withdrawal from the Constitution of the WHO.
On Argentina, the WHO report said", “…the conclusion may be drawn that the purported notification of withdrawal by Argentina should not be accepted as effective.”
Member states are expected to discuss and address the matter on U.S. withdrawal, and is an “open question” according to top officials at WHO.
At a recent press briefing, Steven Solomon, WHO’s Principal Legal Officer said:
“In 1946, the drafters understood the historic struggles against the international spread of disease, and they saw how a truly universal organisation would make the world safer, so they did not include a withdrawals clause….Instead, they provided flexibilities within the treaty so it could accommodate all countries.” (The UN Charter also does not include a withdrawal clause, given the principle of the importance of universality, he said).
On the U.S. withdrawal, DG Tedros Adhanom Ghebryesus said earlier this month: “It is not really the right decision. I want to say it bluntly, because I believe there are many things that are done through WHO that benefit the US. The US cannot be safe without working with WHO”
“The announcement by the United States of America of its intention to withdraw from WHO triggered the immediate termination of several voluntary contribution agreements,” WHO said in reports to the board.
On January 22, 2026, the U.S. Mission in Geneva sent this communication stating that the U.S. withdrew from the WHO “freeing itself from its constraints”: Termination of U.S. Membership in the World Health Organization (WHO) Joint Statement by Secretary of State Rubio and Secretary of Health and Human Services Kennedy.
In the acerbic statement, the U.S. administration said: “Even on our way out of the organization, the WHO tarnished and trashed everything that America has done for it. The WHO refuses to hand over the American flag that hung in front of it, arguing it has not approved our withdrawal and, in fact, claims that we owe it compensation. From our days as its primary founder, primary financial backer, and primary champion until now, our final day, the insults to America continue.”
On Saturday, January 24, 2026, the WHO responded to allegations made by the U.S.:
“…WHO takes note of statements from the government of the United States that say WHO has “trashed and tarnished” and insulted it, and compromised its independence. The reverse is true. As we do with every Member State, WHO has always sought to engage with the United States in good faith, with full respect for its sovereignty.”
WHO also said: “We hope that in the future, the United States will return to active participation in WHO. Meanwhile, WHO remains steadfastly committed to working with all countries in pursuit of its core mission and constitutional mandate: the highest attainable standard of health as a fundamental right for all people”
ON EMERGENCIES
One of the hardest hit areas on account of the financial crisis has been WHO’s emergencies work.
The Board has been asked to guide WHO on the following challenges:
How can WHO strategically prioritize its efforts and foster collaborative partnerships to address the diverse health security needs of countries, particularly in regions facing complex humanitarian crises, while navigating current financial constraints? How can WHO balance immediate emergency response needs with sustained investment in health security systems to build resilience to future crises?
The year 2025 registered the following crisis according to the report covering the period 1 January to 1 October 2025, on all WHO-graded acute and protracted emergencies. It also outlines global health emergency trends, challenges and short- and medium-term outlooks.
Excerpts from the report:
- “Active acute and protracted graded emergencies:
WHO responded to 43 emergencies in 74 countries and territories: 20 Grade 3 emergencies requiring the highest level of Organization-wide support, and 23 Grade 1 and Grade 2 emergencies.
Under the International Health Regulations (2005), WHO scans and triages thousands of signals daily to detect potential public health events of international concern. More than 25 000 raw signals on potential public health events were assessed and triaged. Globally, 351 events were reported, all of which were the subject of an initial risk assessment. (This excludes global emergencies such as dengue, coronavirus disease (COVID-19) and mpox.)
- Global trends
All WHO regions were affected by health emergencies including two Grade 3 emergencies involving two or more regions. WHO has been responding to 10 acute and 10 protracted Grade 3 emergencies.
The escalating climate crisis has an impact on global health, particularly in humanitarian settings. Extreme weather events such as flooding, droughts and cyclones have contributed to widespread malnutrition, disease outbreaks and displacement. Climate-related events are an exacerbating factor for more than 75% of the acute and protracted Grade 3 emergencies.
In 2025, donor cuts triggered a contraction in global humanitarian action. The Emergency Relief Coordinator of the United Nations Office for the Coordination of Humanitarian Affairs launched the “humanitarian reset” to reorganize the humanitarian system and reprioritize resources.
The Global Humanitarian Overview 2025 was revised, and “hyper-prioritized” 43 million of the 81.4 million people targeted for health assistance, reducing the funding requirement by 33.4%, from US$ 3.19 billion to US$ 2.13 billion.
Funding cuts directly affected 5687 health facilities across 20 humanitarian settings, including 2038 that suspended operations, reducing access to services for 53.3 million people (65% of the 81.4 million people targeted for humanitarian health assistance). Funding cuts placed 73% of Health Cluster human resource capacity at risk, undermining coordination and joint and equitable service delivery within countries.
Sixty per cent of women’s organizations have reduced their services. In Afghanistan, Sudan and Yemen, the loss of support to United Nations Population Fund programmes has left over 2.2 million women without access to critical health services. In the eastern Democratic Republic of the Congo, funding cuts have forced the cancellation of 100 000 post-rape kits.
Disruptions to nutrition services are expected to affect 14 million children, including more than 2.4 million who are already suffering from severe acute malnutrition.
Funding cuts have deprived almost 750 000 people of mental health services across 32 countries. As at September 2025, country requests for psychotropic medications in emergencies dropped by 94%, leaving nearly 2 million people without essential treatment.
In 2025, WHO verified 941 attacks on healthcare facilities across 16 countries and territories, directly resulting in 1224 deaths and 892 injuries among health workers and patients. The proportion of inactive facilities is more than eight times higher in conflict-affected areas.
During the reporting period, WHO has responded to major disasters, including earthquakes in Myanmar and Afghanistan, cyclone Jude (Mozambique), typhoons Ragasa and Bualoi (Western Pacific), and extensive flooding in Pakistan…Globally, disaster costs now exceed US$ 2.3 trillion annually when cascading and ecosystem impacts are included.”
PART II: FINANCING CHALLENGES AT WHO
The Programme, Budget and Administration Committee of the Executive Board Forty-third meeting will convene next week 28–30 January 2026.
It will consider member state-led governance reform; timeline for proposing resolutions and decisions; secretariat Implementation Plan on reform; cost recovery mechanisms for voluntary contributions; process of handling and investigating potential allegations against WHO Directors General among other agenda items.
Financing Updates to the EB:
Financing and implementation of the Programme budget 2024–2025 and outlook on the Programme budget 2026–2027
Headed to a billion-dollar gap for 2026-2027.
Projected available funds for 2026-2027 total US$ 3.2 billion, which is 75% of the approved US$ 4.26 billion base segment of the Programme Budget.
This projected financing level is higher than at the same point in previous biennia (75% now vs. 58% at the same stage in the previous cycle). “This is partly because the Programme budget 2026–2027 is lower than the approved Programme budget 2024–2025. US$ 3.2 billion would have meant a 64% expected financing of the 2024–2025 approved Programme budget. However, expected voluntary contributions have also increased in absolute terms. This is the result of efforts led by the WHO Secretariat and Member States to increase the predictability of funding, especially through the investment round. While increased predictability of funding is a positive development, it also means that contributions which, in previous years, would have come in gradually until the start of the biennium have been front-loaded.”
“Given the highly constrained financial environment, closing the remaining funding gap for 2026–2027 will likely be more challenging than it has been in previous bienniums. In addition, it is crucial that future voluntary contributions are aligned with the Programme budget, to address pockets of poverty across major offices and programmatic areas.”
“While it is anticipated that the remaining funding gap will primarily be addressed through specified and thematic contributions, this development places WHO in a stronger position to promote more equitable allocation of resources across outcomes and major offices. This approach not only supports the closing of the funding gap but also advances efforts to improve the distribution of funds, thereby contributing to a more balanced Programme budget funding heatmap.”
“Despite improved predictability and early pledges, mobilizing the remaining US$ 1 billion and with alignment needed to fully fund the budget is expected to be more challenging than in past biennia…it is clear that mobilizing the remaining US$ 1 billion, which is also aligned with Programme budget needs, will be more challenging than in the past. Ensuring more flexible voluntary contributions will be essential to better align financing with the programmatic requirements of the Programme budget.”
- Projected available funds for the 2026–2027 biennium are as follows:US$ 1103 million in voluntary contributions from upcoming agreements (“pipeline”). This includes agreements that are at an early stage of negotiation, as well as agreements for which negotiations are well under way.US$ 574 million in funds from agreements that have already been signed. This includes estimated carry-over from the current biennium, as well as some pledges from the investment round that have already been converted to agreements.US$ 1074.7 million in assessed contributions. US$ 460 million in administrative support funds, from programme support costs collected in 2024–2025.(“The future funding pipeline is defined as proposals that are at advanced stages of development or currently under negotiation with contributors to support the Programme budget 2024–2025”)”
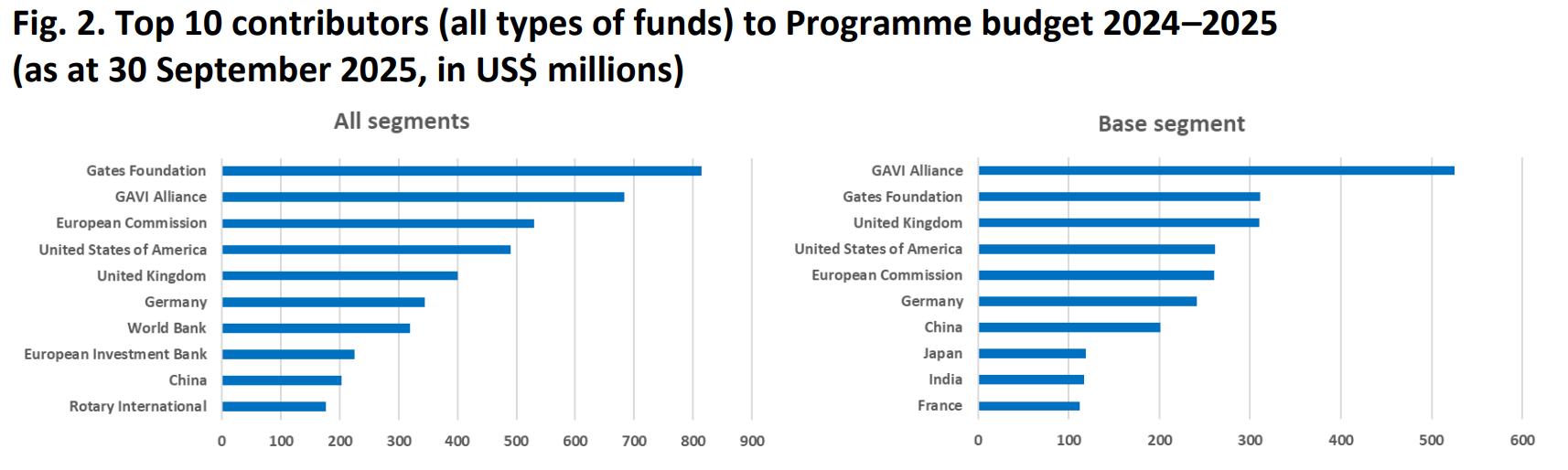
- On the previous biennium, WHO said: “In 2024–2025, the top 10 donors provided 57% (US$ 4.2 billion) of total available funds, with their share rising to 58% (US$ 2.46 billion) for the base budget…. The funding gap from the non-payment of United States contributions could not be offset directly, as available funds are largely earmarked.”
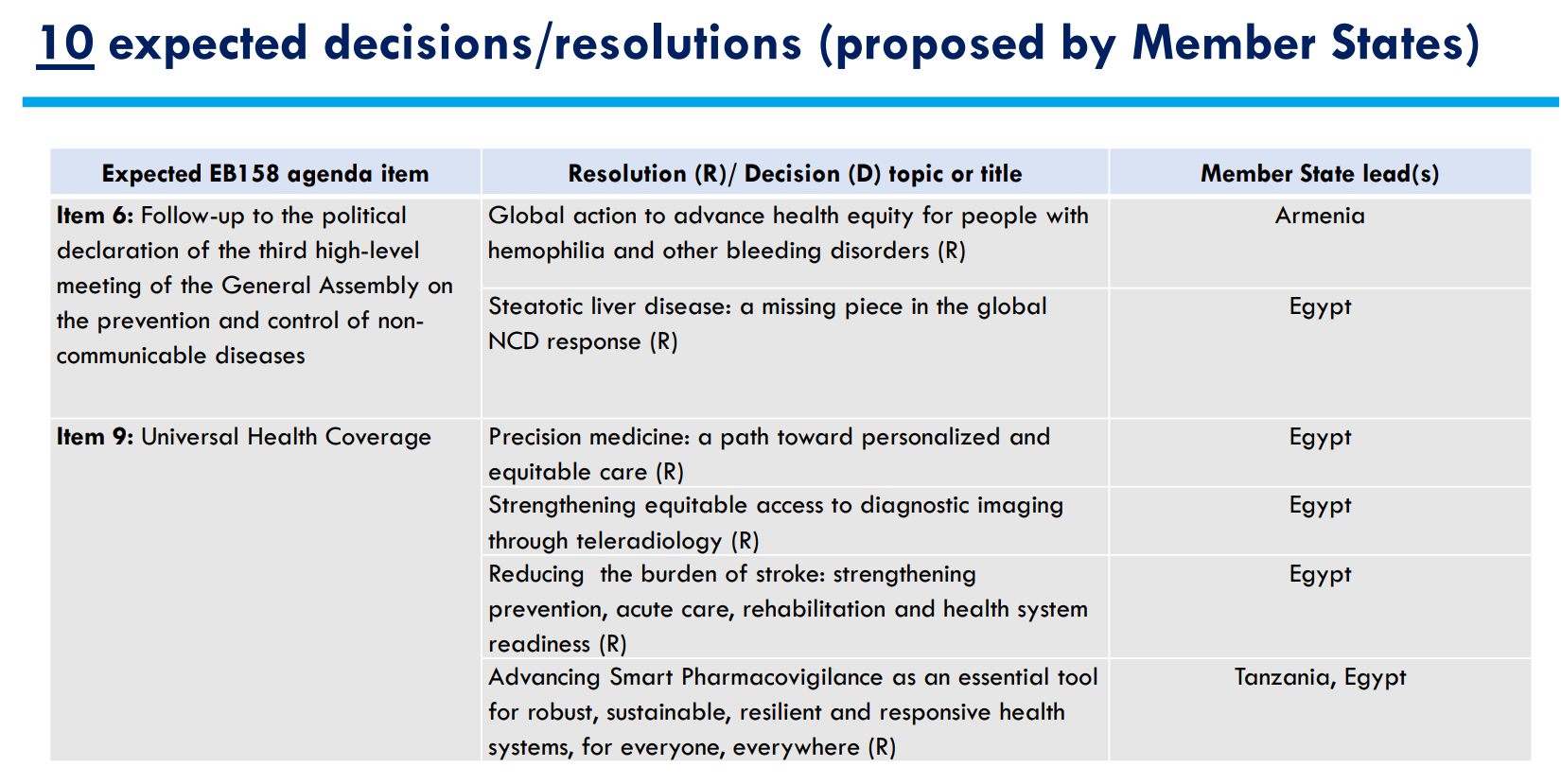
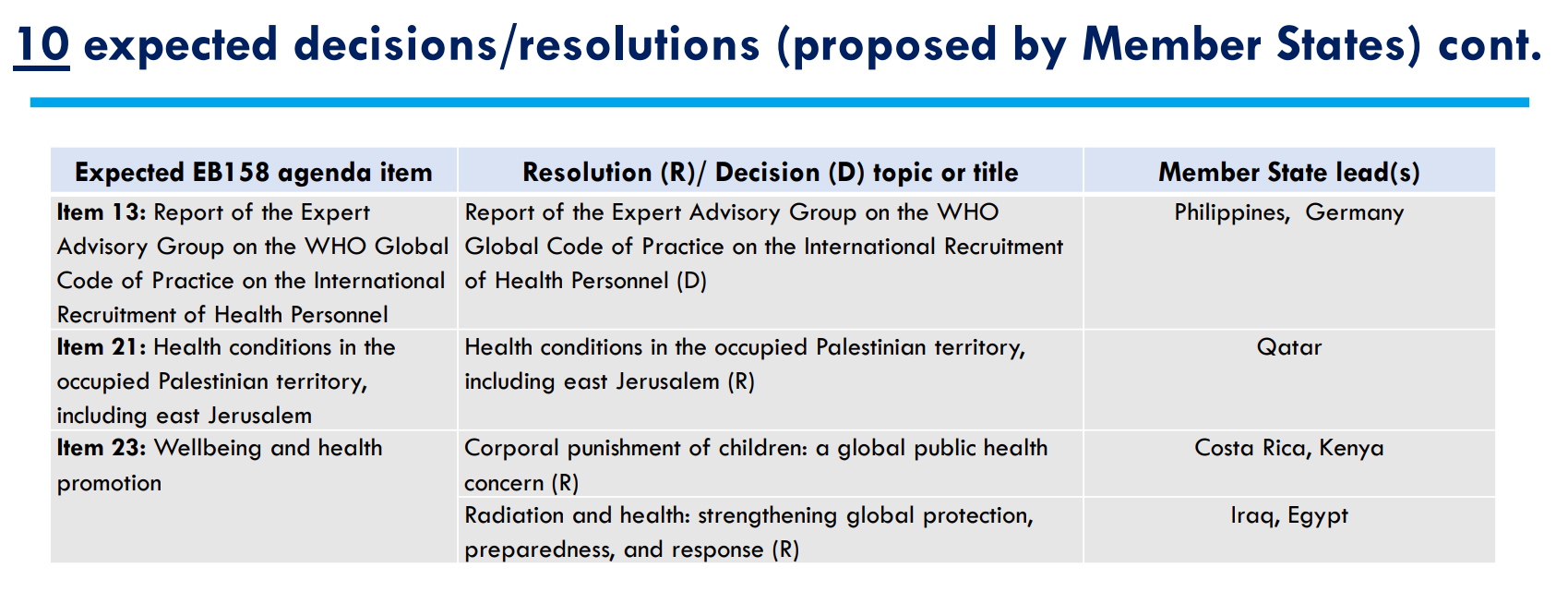
RESOLUTIONS AT THE EB
GOVERNANCE REFORMS
The board will also consider a report on member state-led governance reform. The objective is to ensure a sustainable model for Member State engagement in governance reform. This follows the work of the Agile Member States Task Group on Strengthening WHO’s Budgetary, Programmatic and Financing Governance (AMSTG).
According to the report, such a model of engagement, “…acknowledges the importance of maintaining the agency of Member States, positioning them in a central role for governance reform rather than surrendering leadership on implementation, monitoring and review to the Secretariat or others.”
Other reforms include improvements to the process for proposing draft resolutions and decisions, and efforts to implement the agreed process for handling and investigating potential allegations against WHO Directors-General.
TAIL PIECE: WHAT WAS NOT INCLUDED
- Item on health in conflict and displacement settings
- Item on strengthening measurement of health and health-related Sustainable Development Goals in conflict-affected settings and mobile population
- Item on strengthening event-based surveillance and epidemic intelligence from open sources
- Item on corporal punishment as a public health concern
- Item on safeguards for engagement with advocacy litigants in official relations under the Framework of Engagement with Non-State Actors
Great that you love our work. However, forwarding exclusive editions hurt us and directly undercuts our work. Please ask your friends and colleagues to become subscribers. It helps us show up when the going gets tough. Thank you for understanding.
Also from us:
 Priti Patnaik
Priti Patnaik Priti Patnaik
Priti Patnaik Priti Patnaik
Priti Patnaik
Global health is everybody’s business. Help us probe the dynamics where science and politics interface with interests. Support investigative global health journalism.

![Developing Countries Get More Time to Negotiate Language on Technology Transfer To Fight Anti-Microbial Resistance [WHO EB158 UPDATE]](/content/images/size/w960/format/webp/substack-post-media-s3-amazonaws-com/public/images/619783d3-b5b5-4cc1-8707-703eded46016_7957x5968.jpg)
![[GUEST ESSAY] When Alcohol Disappears From Accountability on Non-Communicable Diseases, Prevention Loses [EB158 WHO]](/content/images/size/w960/format/webp/substack-post-media-s3-amazonaws-com/public/images/76e70ede-eb1b-4162-bc23-c9048136a26f_3840x2160.jpg)

